Clinical Documentation Integrity (CDI) requires a comprehensive, multidisciplinary, hospital-wide effort to incorporate the terminology needed to accurately translate a patient’s condition into precise codes. A robust CDI program will improve healthcare record documentation, which in turn ensures improved patient outcomes, appropriate data quality scores, and accurate reimbursement. Ideally, a CDI program results in more meaningful patient information and data. According to the American Health Information Management Association (AHIMA), “In order to be meaningful, the documentation must be clear, consistent, complete, precise, reliable, timely, and legible to accurately reflect the patient’s disease burden and scope of services provided.” 1 The Golden Rule for physician documentation is, “If you didn’t write it, it did not happen.”
The American Hospital Association (AHA) reports that there were over 36 million total hospital admissions in the U.S. for 2019. 2 While the Centers for Disease Control and Prevention (CDC) notes, “in 2016, there were an estimated 883.7 million office-based physician visits in the United States.” 3 Research shows that on average 45% of patient medical records contain documentation that is of poor quality. This means each year about 414 million patient record entries are created that contain poor-quality clinical documentation. These statistics are alarming and demonstrate the need to develop a strong CDI team within your organization. 4 5 Considering current labor shortages, the ability to build or expand a CDI team can be challenging. Additionally, CDI and coding professionals may experience professional and personal challenges, such as burnout, mental distress, and childcare issues that can impact staffing. To overcome these issues, many healthcare organizations are turning to technology to help streamline efficiencies and accomplish more with fewer resources. As stated by the Association of Clinical Documentation Improvement Specialists (ACDIS), “The advancement of technology has opened the door to streamline CDI initiatives, and when implemented effectively, it can reduce the administrative burden on providers and achieve high-quality documentation. CDI professionals often work in partnership with technology products and vendors to improve clinical documentation” 6
At AGS Health, we work with over 100 healthcare providers across the US, providing customized solutions that marry technology and data analytics with medical coding and CDI services. Provided below is an overview of the top CDI trends we observed while analyzing internal coding and documentation efforts performed by one of our largest customers in 2021. The organization has a very mature CDI program with clearly defined policies, procedures, physician query templates, education programs, and electronic CDI tools.
Physician Queries Deep Dive
For this customer, we provide both concurrent and retrospective CDI reviews for both facility inpatient and outpatient encounters. In 2021, we placed over 200,000 physician queries with approximately 97,000 queries being placed concurrently and the remaining 130,000 queries placed retrospectively.
- For the physician queries issued, 35% of the queries had the potential to impact the principal diagnosis code assignment.
- In 2021, our CDI team identified around 82,000 physician query opportunities that, if answered favorably by the physician, could result in an additional secondary diagnosis that Centers for Medicare & Medicaid Services (CMS) classifies the diagnosis as a major complication and comorbidity (MCC) or a complication and comorbidity (CC) condition. If CC/MCC capture is improved, that will also increase the organization's case-mix index and, therefore, its reimbursement.
- We also initiated over 14,000 physician queries that could help accurately capture the severity of illness (SOI) and risk of mortality (ROM). The addition of SOI and ROM provides an accurate evaluation of both resource use and outcomes.
- Nearly 3% of our physician query volumes were seen with verifying surgeon documentation to accurately assign the ICD-10-PCS or CPT procedure code.
We have observed that 20% of the accounts are pended for physician queries due to unclear documentation. It takes an average of 7 days for the physician to respond to the physician query, which significantly impacts the time it takes to final code and complete the billing cycle for an encounter. Lastly, 42% of the time the MS-DRG has changed due to the query response. The absolute difference in reimbursement cost was close to $9.8 million per month when the MS-DRG was changed post query response.
Types of Physician Queries
In over half of the physician queries initiated, we utilized a physician query form referred to as a general or other specificity query form to clarify the physician documentation. These forms are utilized only when no other specific query form is available (i.e., Renal Status, Malnutrition, etc.) for that diagnosis or procedure. For both the general query form and the specificity query form, these forms are used when signs and symptoms exist for a disease process that is not clearly documented but meets the definition for reportable diagnosis.
Example: A patient was admitted with a symptom of chest pain. Testing performed by the hospital showed findings of peptic ulcers, gastroesophageal reflux, and gastritis. It was also noted in the physician documentation that the patient had severe anxiety and was seen by behavioral health while in the hospital. The patient was discharged home on a new prescription of benzodiazepines, antibiotics, and proton-pump inhibitors. At the time of discharge, the physician did not clearly define the reason for the chest pain. A query is issued for the underlying cause of the chest pain (i.e., ulcer, reflux, gastritis, and/or anxiety). Dependent upon the physician’s response, this could impact the principal diagnosis and ultimately the reimbursement for this patient.
Other notable clinical documentation improvement initiatives were seen by verifying the following diagnosis:
- More than 13,000 queries were initiated because the record reflected extensive clinical indicators for the diagnosis and/or acuity of malnutrition. The degree/severity of malnutrition (i.e., moderate, mild, severe) is a part of the diagnosis of malnutrition, which can only be made by the provider. As detailed in the CMS Official Guidelines for Coding and Reporting, "Code assignment is based on the documentation provided by a patient's provider (i.e., a physician or other qualified healthcare practitioner that is legally accountable for establishing the patient's diagnosis)." 7
- Approximately 6% of our physician query volume revolved around confirming the diagnosis of sepsis and if the diagnosis of sepsis was present on admission. According to the AHA Coding Clinic, Fourth Quarter 2003, pages 102-103 “If the documentation is unclear as to whether the patient is septic, query the provider for clarification. Facilities should work with the medical staff to improve physician documentation and address any documentation issues.” 8
- We issued a conflicting diagnosis physician query around 11,000 times during 2021. This physician query is used when physician documentation conflicts with a particular diagnosis or procedure. For example, the attending physician refers to the respiratory condition as respiratory failure and the pulmonologist refers to the condition as respiratory distress. This is conflicting documentation. As explained in the AHA Coding Clinic, First Quarter 2004, pages 18-19, "Code assignment may be based on other physician documentation (i.e., consultants, residents, anesthesiologist, etc.), as long as there is no conflicting information from the attending physician." If documentation from different physicians conflict, seek clarification from the attending physician, as they are ultimately responsible for the final diagnosis. 8
- Over 8,500 physician queries were used to clarify the diagnosis of heart failure. CDI staff were working with the physicians to further clarify the type and acuity of congestive heart failure.
- Close to 7,500 physician queries were issued in 2021 to determine if the patient has a renal condition, such as acute renal failure, acute renal insufficiency, or chronic kidney disease.
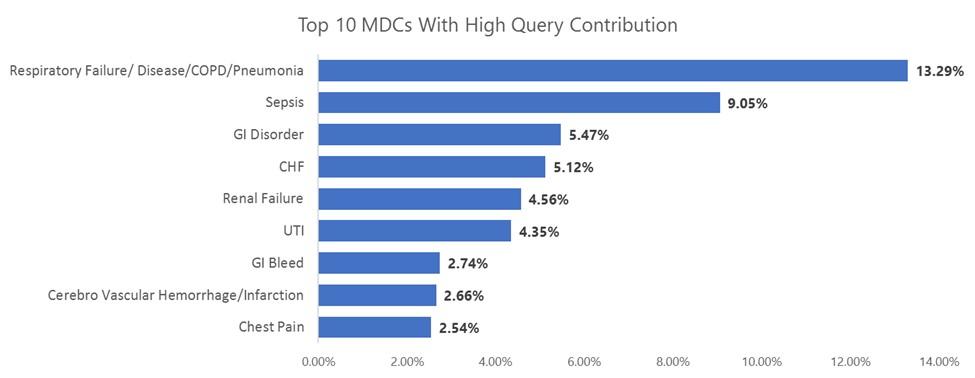
- There were 10 Major Diagnostic Categories (MDCs) that contributed to 50% of queries raised during the last 6 months. Within the 10 MDCs, Respiratory Failure/Disease/COPD/Pneumonia contributed to roughly 13% of queries and is the top area with conflicting documentation.
Clinical Documentation Improvement Recommendations
Clinical documentation improvement is a team effort at all facilities. Clinical documentation is the key to obtaining accurate and specific code assignments to reflect the severity of illness for the patient. Key next steps for your organization to ensure an effective CDI team:
- Create a clinical validation review process for your facility.
- Develop hospital- or facility-specific clinical criteria for high-volume diagnoses such as sepsis, congestive heart failure, and malnutrition.
- Stay current with ACDIS and AHIMA guidance related to compliant query practice and clinical validation efforts.
- Collaborate with various departments to develop effective clinical validation processes.
- Conduct successful physician education related to clinical validation.
If labor shortages or other challenges are hindering your ability to fulfill these recommendations and achieve your CDI goals, AGS Health is available to help. With numerous levels of service, a variety of technologies, and expert services readily available, we are fully equipped to support your CDI needs. To speak with a representative, please contact us at info@aghealth.com.
References:- American Health Information Management Association. (2022, March). Education & events
- American Hospital Association. (2022, March). Fast facts on U.S. hospitals, 2022
- Ashman, J. J., Ph.D, Rui, P., M.P.H., Okeyode, T. (2019, January). Characteristics of Office-based Physician Visits, 2016. Centers for Disease Control and Prevention.
- Bowman, S., MJ, RHIA, CCS, FAHIMA. (2013, October 1). Impact of electronic health record systems on information integrity: Quality and safety implications. National Library of Medicine.
- Bryant, G., RHIA, RHIT, CCS, CCDS. (2010, June). The physician query process & compliance issues. HCCA West Coast Regional Conference. Newport Beach, CA.
- Association of Clinical Documentation Improvement Specialists. (2021, December 9). News: ACDIS/AHIMA Compliant CDI Technology Standards position paper released
- Centers for Medicare and Medicaid Services. (2019). ICD-10-CM official guidelines for coding and reporting FY 2019
- American Hospital Association. Coding Clinic

Leigh Poland RHIA, CCS
Author
Leigh has over 20 years of coding experience and has worked in the coding and education realm over the last 20 years. Her true passion is coding education making sure coders are equipped to do their job accurately and with excellence. Academically, Leigh has graduated from Louisiana Tech University with a Bachelor of Science. Leigh has had the opportunity to present many times in the past at the AHIMA, ACDIS, and AAPC National Conventions. She has been a guest speaker on AHIMA webinars and has written several articles that were published in the AHIMA Journal. Leigh has traveled the US and internationally providing coding education.